Child Mortality in Southern Sudan By Augustino Mayai
Abstract Using the 2006 Sudan household sample and representative data of 455 women and 1,490 live births from two southern states and UN death estimate from Darfur, child mortality patterns are assessed. This paper uses a multivariate analytic framework, including relative measurements and indirect demographic regressions to evaluate these childhood mortality patterns. Results are consistent with the posed hypotheses. Sudanese childhood mortality rates were comparatively higher during conflicts but lower in the absence of conflicts, and were relatively higher in the south, compared to the rest of the Sudan, including Darfur. I conclude with a policy-oriented remedy, that childhood survival in the Sudan may be improved through considerable reductions in civil conflicts, instability, and inequality in human service distribution—factors that are crucially associated with childhood survival in the polity.
Since the 1940s, substantial declines in infant and child mortality rates have taken place in most developing nations (Hill & Pebley, 1989). This decline in childhood mortality is attributed to improved standards of living, scientific advances, and improvements in national and international public health intervention programs. Childhood mortality in the developing world is highly correlated with preventable health problems, such as underfeeding and infectious diseases, phenomena inextricably linked to underdevelopment. But for nations experiencing conflicts—the majority of which are extremely under-developed—direct and indirect influences of civil violence become additional sources of death among the most vulnerable populations, such as children, women, and the elderly. The global child mortality rate in 2006 was estimated at 72 deaths per 1,000 live births (UNICEF 2008). In Sub-Saharan Africa, in 2006, 1 in every 6 children dies. In Southern Sudan, 1 in every 4 children dies (Guha-Sapir et al., 2005). The aim of this study is to explore the influence of conflict and conflict-related factors on childhood mortality in Southern Sudan. To fully understand the patterns of childhood mortality in Southern Sudan, I use the state of Darfur as a central point of reference, though other regions of the Sudan are introduced in making similar illustrations. This research has important policy and practical implications for Sudan as a whole and Southern Sudan in particular. The research findings could be used to help address the issues of conflicts, instability, social inequality, and health problems that continue to confront the highly vulnerable Sudanese rural populations, such as children, women, and the elderly. In addition, the research provides scholarly insights into health conditions affecting the population of Southern Sudan following peace, while serving as an important point of departure for future demographic studies. The rest of the paper covers the following segments. Segment II describes the study; segment III reviews related literature; segment IV reviews data materials; segment V describes the empirical and analytic frameworks; segment VI presents the concise backgrounds of both the Sudan and Southern Sudan; segment VII presents the results; and VIII concludes.
This timely and important study examines childhood mortality levels in the Sudan, with primary emphasis on Southern Sudan. Two central questions are addressed. First, I assess South Sudan’s childhood mortality levels before and after the conflict, and, based on historical evidence, speculate upon underlying causes, while making recommendations for the future. Second, though within-regional variations are emphasized, I explore child mortality differentials between Southern Sudan and Darfur. I compare Southern Sudan with Darfur to indirectly explain the differential effects of civil conflict on childhood mortality across these two regions. Thus the following two hypotheses are investigated. Hypothesis 1. This hypothesis seeks to answer whether Southern Sudanese child mortality rates were higher in periods of violent conflict than in peaceful periods. Because violence directly or indirectly causes deaths, destroys the economy and healthcare, uproots social networks, and lowers the standard of living for the population, I predict that child mortality rates in Southern Sudan were higher during the period of protracted conflicts (1990-2005) than in times of peace (1972-1983 and 2005 to the present). Hypothesis 2. This hypothesis seeks to answer whether, within Southern Sudan or between Darfur and Southern Sudan, there are discernible differences in child mortality rates, depending on their relative development levels and a number of other factors. A relatively well-built infrastructure, including greater availability of public services and private markets may increase the levels of childhood survival. Because Central Equatoria state, not Warrap state, is relatively more developed, is the center for the southern government, and has greater access to both international and local markets, I expect better living conditions there. Therefore, I predict that childhood mortality rates will be higher in Warrap State than in Central Equatoria State. Similarly, because Darfur, but not Southern Sudan, has substantial remnants of historical development and was somewhat politically and economically advantaged until recently, I predict that childhood mortality rates in Darfur are likely to be comparatively lower than in Southern Sudan.
In 1990, Roth and Kurup assessed the levels of childhood mortality in two southern towns, Wau and Juba, investigating the effect of UNICEF’s health care program in the region. They found that the cumulative probability of dying for Southern Sudan’s children ranged from a little over 14 percent (by age 1) to over 31 percent (by age 20). These rates reflect disease severity and probability of dying before a certain age for a cohort member (Guha-Sapir et al., 2005). Preston and Farah (1982) studied child mortality differentials in Sudan using the 1955/6 and 1973 census data. According to the 1955/6 census results, the probability of dying by age 5 in Southern Sudan was estimated at about 26 percent, compared to 15 percent in Darfur, nearly 15 percent in the North, and 18 percent in the whole Sudan. The 1973 census results show that the probability of dying in the Southern region was 23 percent, compared to 14.8 percent in Darfur, 14 percent in the North, and 17 percent in the whole Sudan. Although there seemed to be a modest decline of child mortality in all Sudanese states following the 1955/6 census, evidence demonstrates that the child mortality pattern post-the 1955-6 period remains relatively higher in the Southern region than in other parts of the Sudan. In Southern Sudan, for example, infant mortality was 150 per 1,000 live births; the under-five mortality was 250 per 1,000 people in 2004 (UNICEF). These mortality rates in Southern Sudan come from a period in which the region was in critical civil disorder. Palloni and Hagan (2006) quantified the crude mortality rate in Darfur, with estimates that ran from 70,000 to 255,000 deaths between 2003 and 2006. Those death numbers are largely associated with direct violence and forced migration. Due to the issues of data quality, the authors failed to estimate infant and child mortality, relying exclusively on regional crude mortality. Prior research has documented that most deaths, including early childhood deaths, in Southern Sudan, are related to violence and malaria pandemics. For example, according to Preston and Farah (1982) millions of citizens from the Sudan suffer malaria-related illnesses each year. Their study also showed that nearly one million malaria related cases were treated in Sudan in 1974—a majority of them children*. In the State of the World’s Children, UNICEF (2008) finds that some 26,000 plus children under the age of five die daily around the world from preventable causes, conflicts included. This finding also suggests that nearly all the children who are affected live in the developing world. A number of studies indicate a well-established causal link between conflicts, malnutrition and diarrhea among children in Southern Sudan. Poor feeding in younger children leads to impaired immune systems and can cause, among other effects, severe diarrheal diseases, resulting in a higher susceptibility to mortality associated with diarrhea in the group (Rice et al., 2000). A recent Southern Sudan case study by Guha-Sapir and others (2005) relates internal displacement and death. Their results show that childhood mortality associated with bloody diarrhea and malnutrition epidemics was around 16 per 10,000 per day in June 2002 in the southern state of Jonglei. Such childhood mortality rates were also influenced in part by nature driven and war induced events, such as low crop production in the area because of drought, flooding, and bird attacks Guha-Sapir et al (2005). In a related publication, Guha-Sapir and colleagues (2005) report that the average acute malnutrition rate for children, amid violence, was 35 percent in Jonglei and Bahr El Ghazal states, a measure more than twice the national average of 16 percent between 2001 and 2003. In general, prior research based on cross-sectional data illustrates that the major causes of death in Southern Sudan and Darfur are closely linked to intermittent civil wars. In addition, this research also links civil conflicts with a greater prevalence of infectious and parasitic diseases, respiratory ailments, malnutrition, famine, and poverty among persons of relatively younger ages.
Data for this research come from Southern Sudan and from other states of the Sudan. There are two data samples collected in two southern states, Warrap and Central Equatoria in 2006 and 2007, respectively. The data contain information on the total number of children born and children dead to women aged 15-49. Together, the two survey waves make up a convenient sample of 455 mother participants and 1,490 live births. There were 869 live births recorded in Warrap and 621 in Central Equatoria. Of the total, 287 or 19 percent of the children were reported dead. The proportions of children dying in Southern Sudan were approximately 21 in Warrap and 17 in Central Equatoria. Both sample data present total fertility rates of 3.3 in Southern Sudan; 2.4 in Central Equatoria; and 4.4 in the more rural state of Warrap. These data provide retrospective birth and death information for children aged 1 and older, which is used to assess the child mortality regime in the region. Since mothers do the reporting of these data, only children of surviving mothers are sampled, causing a potential downward bias in the estimator. The other dataset is the Sudan’s 2006 household weighted data comprised of about 20 million individuals. The data were collected and analyzed as part of the development exercise funded by USAID and supported by the Sudanese government. The survey contained two forms: short and long. The present data come from short forms, which became available shortly after the survey because they were easy to analyze. This dataset is larger than the Warrap and Central Equatoria samples combined, and is representative of an estimated 25,000 households from all 25 Sudanese states. These data contain information on demographic characteristics of the households, such as sex, age, level of education, social class, health services such as water, sanitary facilities, antenatal care, immunization, available health clinics, and the states from which the households were drawn. I use these data to evaluate the factors that may account for child mortality differentials across Sudanese states. Health services, for example, are used to illustrate why child mortality regime in one state may be lower than in another state. Although Darfur is represented in the 2006 household data there are no child mortality representative data for all ages as shown in Warrap and Central Equatoria States. Rather, I use the 2004 UN/WHO estimates of under-five mortality in Darfur to assess the regional childhood mortality pattern within this particular age range.
The first component of this analysis demonstrates the extent to which indicators of childhood mortality in the Sudan differ across Sudanese states, especially among South, North, and Darfur. Specifically, I evaluate how development and mortality indicators, such as health services, differ across these regions. I compare regional development and mortality indicators using cross-tabulation and relative measure techniques. In particular, I present development and mortality indicators using proportions, relative measures, such as odds, index of dissimilarity, coefficient of variation (V), and chi-square statistics. The second component of the analysis uses indirect analytic strategies of child mortality estimation to analyze the indicative levels of childhood mortality in the studied regions of Sudan. Brass and colleagues’ 1968 indirect methods of childhood mortality estimation use data from the average number of children ever born and average number of children surviving per woman, tabulated by age specific groups of women in a population. The regression equations—relating the multipliers to the indices of fertility patterns—are borrowed from Coale-Demeny’s north family life-table. But note that the Brass’ analytic methods are only instrumental with respect to some of the data collected in southern region, depending on the nature of the information contained in those data. The level of child mortality q(x) is parameterized, so that
where qx is the probability of dying between birth and age x, alpha, beta, and delta are life-table coefficients, P(s) denote parity ratios; the first three parts of the equation to the right form an age-specific factor called Mi, and Di, the reported proportion of children dead at exact age x to women in age group (x, x+5). I caution that probabilities estimated using indirect methods need not be interpreted as actual death rates. Rather, they serve as indicators of potential, if not, hypothetical mortality levels of children of a given population. They are simply a product of life table multipliers and actual death proportions drawn from real data. The probabilities of dying between birth and exact ages q(x) in Southern Sudan are estimated using the United Nations’ Mortpak Software. The average number of children ever born and average number of children surviving per woman, specified by age groups of mother, are entered into the Mortpak program in order to obtain the desired estimates. Prior to the results, I first present a concise background of both Sudan and Southern Sudan.
Sudan is the largest African nation, with a comparatively small but rapidly growing population. The name “Sudan” derives from the Arabic bilad as-Sudan, “land of the blacks.” The Sudan was under political domination of both Great Britain and Egypt. Contacts between Egyptians and the African people living along the southern banks of the Nile, the today’s northern Sudan (Nubia), occurred ‘as far back as Stone Age’ (Petterson, 2003). The continued interrelationship between Egypt and Nubia caused an influence on each other’s art, culture, economy, and religion. Sudan gained independence in January of 1956 but faced numerous internal frictions thereafter. The first internal tension pitted the southern Anyanya rebels against the northern regime. Although a peaceful settlement between the two Sudanese warring rivals was attained in 1972, still decades of intensive disorder inaugurated ten years later. Religion, race, power, and oil have had significant influences on Sudanese civil conflicts. The 1980 discovery of oil in Southern Sudan, for instance, worsened the south-north relationship, especially when the ‘Nimeiri administration immediately sought to maximize central government control over resources’ (Petterson, 2003). The bill proposed in 1980 by the administration set new regional boundaries between the south and the north, with oilfields originally in the south redrawn to the northern territory. Great dissatisfaction that eventually led to 1983 southern rebellion detonated when the Sudanese president Jaafar Nimeiri insisted to institute policies that disfavored the south, including the use of his tribal Arab militias to potentially exterminate Africans of the region (Jok, 2007). Southern Sudan is comprised of ten states, including Lakes, Warrap, Jonglei, Central, Eastern, and Western Equatoria, Unity, Upper Nile, West and North Bahr el Ghazal. South Sudan will vote for independence in a referendum that is scheduled to take place in 2011. The region gained a six-year self determination when the Sudan’s central government and the South’s rebel group, the Sudan’s People Liberation Army (SPLA), signed what became the Comprehensive Peace Agreement (CPA) on January 9, 2005 in Kenya. More than 90 percent of the southern region is primarily rural, with the most disabled infrastructure. The inhabitants of South Sudan come from various ethnic/tribal communities, including the Dinka, Nuer, Acholi, Kakwa, etc. South Sudan has an agriculturally suitable land, which is primarily used by these communities for both traditional pastoralism and farming. History shows that the peoples of Southern Sudan, who are mainly Nilotics and African blacks, appear to have been largely isolated from the rest of the country and the world at large. During the years of Ottoman Empire South Sudan was a conduit of slaves. Isolated from the rest of the country for foreign and domestic ruling motives, South Sudan has been enduring acute economic and political deprivations, as state benefits and services controlled in the north remain inaccessible to regional populace (see Jok, 2007). Anguished by northern rulers and their policies of racial, religious, and regional domination, the people of Southern Sudan demanded to be separated from the rest of Sudan in order to escape political, racial, economic, and religious oppressions concerted in the north. Hence, the protracted periods of deadly civil conflicts between the north and the south.
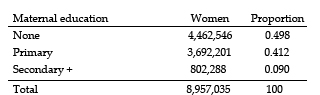
A. Mortality Indicators Summarized Part A presents results from the 2006 household data. This summary analysis demonstrates the extent to which indicators of childhood mortality in the Sudan differ by state/region. Specifically, I summarize how maternal levels of education, antenatal care, childhood vaccinations, and sanitary services differ across regions. First, I organize Sudan into six distinct regions, including South, Darfur, East, Eastern, North, and Central.** Second, I compare regional development and mortality indicators using cross-tabulation and relative measure techniques. Although the results are evaluated on the basis of regional classifications, when the data permit comparisons are made at the household level. I use region as a proxy of determinants rather than a determinant itself. I. Maternal Education in the Sudan Table 1 presents summary statistics of maternal education. Because the present data do not provide information on regional or state level maternal education, my analysis of maternal education only evaluates Sudan as a whole. I find that nearly fifty percent (49.8 percent) of all women sampled in 2006 had no formal education at all, forty-one percent had primary education, and only nine percent had secondary or some form of higher education. Kurup and Roth (1990), Preston (1978), and Caldwell (1979) found significant associations among childhood survival, immunization, oral dehydration, and maternal education. Higher levels of education for mothers have been associated with many household factors, such as knowledge of proper health practices, income levels, sexual balance of power, and access to health facilities (Caldwell 1979). Preston and Farah (1982) find that a unit increase in maternal years of education reduces child mortality by nearly 4 percent.
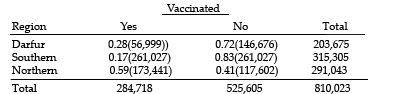
Maternal education across Sudan is quite poor, and the lowest rates seem to be concentrated in the southern region. In Southern Sudan, the estimated literacy rate for female adults is between 10 and 12 percent (UNICEF & NSCSE 2004). The rate is comparatively lower than that of northern Sudan, where the female literacy rate is estimated at 52 percent according to the World Bank (2006). In other words, the authors argue that advances in female education present one of the important means of reducing childhood mortality in the developing world. II. Childhood Vaccination I find significant variations in the levels of childhood vaccination in the Sudan. Childhood vaccination statistics are summarized in Table 2 and Table 3. The data under review show that the proportions of children vaccinated in the Sudan in 2006 were 0.17 in the South, 0.28 in Darfur, and 0.59 in the North. This means that the odds of childhood vaccination in Darfur and Northern Sudan, compared to that of Southern Sudan, are 1.87 and 7.09 times greater, respectively. In the North, the odds of childhood vaccination are 3.78 times greater than in Darfur. The finding is consistent with the hypothesis that Southern Sudan, relative to the rest of Sudan, has the most unfavorable living conditions with respect to development indicators and general distribution of national resources, and has relatively low levels of economic and health resources.
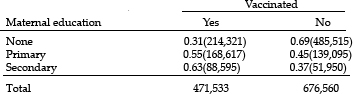
I also find significant differences in the rate of childhood vaccination when associated with mother’s education (see Table 3 below). About thirty-one percent of children born to non-educated mothers are vaccinated in 2006, compared to nearly fifty-five percent and sixty-three percent to mothers with primary and secondary or higher education, respectively.
The odds of childhood vaccination for mothers with primary and secondary or higher education are 2.75 and 3.86 times greater, respectively, compared to that of mothers who had no formal education at all. In addition, the odds of vaccination for children whose mothers reported having secondary or higher education are 1.41 times greater than for children whose mothers had primary education. My data indicate a statistically significant relationship between childhood vaccination and mother’s level of education when I use the chi-square test of independence with 4 degrees of freedom at a 95 percent confidence level (result not shown). This result suggests that childhood vaccination is substantially associated with mother’s level of education among others, with a relatively greater risk of not being vaccinated if the child has a non-educated mother.
In Tables 4 and 5 I examined regional differences in antenatal care. First, I analyzed these differences across three regions: South, North, and Darfur. My results show that about 75 percent of expectant mothers sampled in 2006 in Darfur received antenatal care. Expectant mothers in the North had a greater advantage, with majority or nearly 88 percent receiving antenatal care, while only 40 percent of southern expectant mothers received this service. Expectant mothers who received antenatal care in the North had the odds two times and nearly eleven times greater than their counterparts in Darfur and Southern Sudan, respectively. Similarly, Darfur expectant mothers had better antenatal care services compared to Southern Sudanese expectant mothers, with the odds closer to 4.5 times greater there than in Southern Sudan. A chi-square statistics confirms that these results are statistically significant at a 95 percent confidence level, suggesting that there are discernible differences among these populations (result not reported).
In my second comparative analysis, I consider a more refined regional classification. My new classification emphasizes six distinct Sudanese regions, namely the North, South, Darfur, Kassala, East, and Central. This classification is useful because it helps tease out the extent to which experiences of other regions [but not the north) not attended to in the previous analysis may differ or relate to both Darfur and Southern Sudan. The findings are particularly interesting. When I classify northern Sudan as Khartoum, Northern, and River Nile states (that is, I each group east and northeastern states separately from the north), the proportion of expectant mothers who received antenatal care in Khartoum goes up by nearly 5 points (0.926 vs. 0.88). This finding is striking because it proves that much of the country’s resources appear to be highly concentrated in the hub of Sudanese government, particularly Khartoum. Specifically, the percentage of mothers receiving antenatal care in 2006 were 40 in the South, 74.9 in Darfur, 78.7 in Kassala, 79.5 in East, 83 in Central, and nearly 93 percent in the North. These results are consistent with the previous analysis, indicating that Southern Sudan, compared to the rest of Sudan, receives fewer resources from the central government, is extremely under-developed, and has extreme poor health and economic systems. For instance, when comparing each of the other regions of the Sudan to the South, I find that the odds of a mother receiving antenatal care become 18.7 times greater in the North, nearly 4.5 in Darfur, 5.5 in Kassala or Northeastern, nearly 5.8 in Eastern, and 7.3 in Central than in Southern Sudan. These results are statistically significant on a 95 percent scale (result not shown).
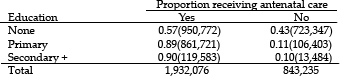
When I analyze antenatal care provision on the basis of maternal educational attainment as shown in Table 5 above, I find that nearly 57 percent of all expectant mothers sampled in 2006—who reported having no formal education—were on antenatal care. This is in relation to 89 percent among mothers who reported having attained primary education and nearly 90 percent among those who attained secondary or higher level education. The odds of antenatal care provision were 6.16 and 6.75 times greater for mothers with primary and secondary or higher education, respectively, than for mothers without any sort of formal education. The results are all statistically different from 1 at a 95 percent confidence level (results not shown). That is, a mother’s education in the Sudan is substantially related to the level of health care services she receives while pregnant.
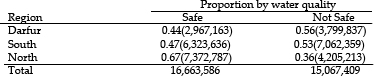
Another important indicator of development and mortality captured in this analysis is the extent of sanitary services across Sudanese regions. This portion of the analysis, whose results are shown in Tables 6 and 7, examines how sanitary services vary across Sudanese regions. Sanitation is very important because poor sanitary conditions have a significant influence on an overall health of individual populations. In most developing and under developed nations, infectious and respiratory diseases—most of which are major killers in these populations—are a product of poor sanitary services, such as lack of latrines and clean, safe drinking water. First, I evaluate the quality of drinking water accessible to the households in the comparable Sudanese regions. Sixty-four percent of the household members sampled in the North had safe drinking water, compared to 44 percent in Darfur and 47 percent in the South, respectively. In the north, the odds of having safe drinking water were 2.25 times greater than in Darfur and 1.96 times greater than in Southern Sudan. The odds of having safe drinking water are 1.15 times greater in the South than in Darfur. This slight advantage of the South in the availability of clean, drinking water is presumably linked to the fact that drinking water facilities in Darfur have been decimated by the conflict which the region has since experienced since early 2003 (Hagan 2009). This modest difference might also result from a number of sampling uncertainties. Despite the fact that other explanations may be relevant in this particular finding, the chi-square statistic (not shown), however, confirms that this particular difference between the two populations is statistically significant, suggesting an existence of real differences between the two regions with regard to this particular situation.
Conducting a test of independence in the overall Sudanese population between the quality of drinking water received by the populations and the region in which they reside yielded a statistically significant result. In particular, a chi-square statistic (not shown) tells us that there is no substantial evidence in favor of the hypothesis that there is no relationship between region of residence and the quality of drinking water available to the household members. That is, the data tell us that region of residence and the kind of drinking water the household members have are substantially related.
In Table 7 above, I summarize the differences in the availability of latrines or toilets to the households. Only 18 percent of the household members in this particular survey reported having either a latrine or toilet in Southern Sudan, compared to 62 and 79 percent in Darfur and Northern Sudan, respectively. These differences are also reflected in the odds such that the extent of availability of a latrine or toilet to a household becomes 2.3 and 16.5 times greater in the north than in Darfur and Southern Sudan, respectively. Similarly, the odds that a household has either a latrine or toilet in the region of Darfur were 7.1 times greater than in Southern Sudan. V. Child Birth: Place and Delivery Method Facility and methods of child delivery, among others, may serve as proxies for understanding children’s well-being. In Sudan, a vast majority of children born in rural areas are not delivered in modern clinics by professionally trained doctors or nurses, unlike in modern towns and cities. The fact that a child might be born in the absence of a medical doctor or adequate medical services in those places implies that a newly born child is at a high risk of infancy or childhood health problems. Children who do not get vaccinated or immunized are more likely to die as infants or children than their counterparts. In addition to the greater likelihood that a child might die during birth, a lack of medical protection against childhood diseases in rural areas due to the absence of quality health facilities further signifies a higher level of child mortality in those settings. Tables 8 and 9 present the methods and facility of child’s birth, respectively. My analysis of assisted child delivery shows that nearly 81 percent of children born in the North get delivered in modern health facilities in presence of a professionally trained medical specialist. This is in contrast with 49 percent in the region of Darfur and a low 30 percent in Southern Sudan. In other words and based on this particular representative sample data, 70 and 51 percent of all child births in Southern Sudan and Darfur, respectively, are attended to by traditional, non-medically trained midwives, and mostly occurring in mothers’ residence, not in medical facilities. These results are not surprising since medical advances are closely associated with general development, which seems to be lacking in both Southern Sudan and Darfur, subject to regional variations. The chi-square statistic indicates that these differences are significant (result not shown). Thus, the hypothesis that there is no relationship between region and the type of child delivery is not supported by the data. In other words, there is a statistically significant relationship between child’s region of birth and the type of assisted delivery given to the mother while giving birth.
Results in Table 9 below indicate that, of the studied three Sudanese regions, Southern Sudan accounts for 43 percent of all child births occurring at home. Similarly, of all children born in primary health care centers and units in 2006, Southern Sudan accounts for 82 and 77 percent, respectively. No hospital deliveries or births were recorded in Southern Sudan in 2006. Instead, a significant proportion (0.99) of hospital related births is found in the north, and the other proportion is in Darfur region.
When I further partition Northern Sudan into North and Northeastern regions, as shown in Table 8 above, the resulting analysis shows that 90 percent of child births in the North take place in modern health facilities and in presence of a medical doctor. Because the North is where most of the national resources seem to be concentrated, it is not surprising that child birth services and related protection in Northeastern Sudan are, on average, low (66 percent) compared to North Sudan. Yet, the average child birth services and protection in Northeastern Sudan are 4.45 and 2 times greater than in Southern Sudan and Darfur, respectively. This refinement of the regions also means that the odds of child birth services in the North become 20 and 9.4 times greater than in Southern Sudan and Darfur, respectively. Finally, I examine the same differences across Central Sudan, Southern Sudan, Darfur, and East Sudan. My analysis indicates that 66 and 73 percent of child births in Central and East Sudan, respectively, take place in health facilities and in presence of professionally trained doctors and nurses. Similar patterns are reflected in relative measures. Thus, the odds of a child being delivered in a modern health facility and in presence of a doctor are 4.6 and 2.1 times greater in Central than in Southern Sudan and Darfur, respectively. For East Sudan, the odds are 6.3 and 2.8 times greater there than in Southern Sudan and Darfur, respectively. These findings are all consistent with the notion that Southern Sudan experiences relatively greater levels of under-development and poor health services than other regions of Sudan.
The differences observed in the above indicators of human services and development among the regions highlight the extent of regional inequality in the state of Sudan. I approach this problem by using the index of dissimilarity (D) to assess the percentage distribution of development and human services in Sudan, particularly across Darfur, Southern, and Northern regions. Initially developed by White (1986) to help measure racial segregation in the United States, the D index is also suitable for studying other distributions. In my case, D takes the following form:
and
where Ni, Si, and Di represent the total percentages of populations receiving relevant human services in Darfur, Northern, and Southern Sudan, and DNS and DDS represent the percentage of those receiving human services that Northern Sudan and Darfur would have to redistribute between them and Southern Sudan in order to achieve equality in the distribution of populations benefiting from available human services in the country. Results are presented in Table 9 below. Table 10. Index f Dissimilarity, 2006 Household Survey
The results are remarkable and are consistent with prior expectations. The average index of dissimilarity between Northern and Southern Sudan is 0.79. In other words, this is nearly 80 percent of human population benefiting from human services in the North than in the South. In order to realize equality with the South, the North would have to redistribute services that flow to the excess 80 percent of its population. This finding affirms my understanding that most Sudanese national resources tend to be concentrated in Northern Sudan. Similarly, the average index of dissimilarity or the excess human distribution receiving human services that Darfur would have to redistribute to ensure equality with Southern Sudan is 0.31 or 31 percent. This finding is interesting, given the current conflict in Darfur, but not particularly surprising because regional inequality since Sudan’s independence has been much more pronounced in Southern Sudan than elsewhere in the country.
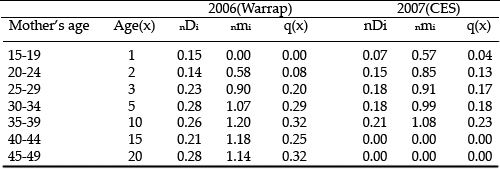
In this section, I present childhood mortality estimates for Southern Sudan and Darfur. Results are based on sample data comprised of 455 mothers (198 from Warrap state in 2006 and 257 from Central Equatoria state in 2007) with total 1,490 births (869 and 621, respectively), and the 2004 UN estimate in Darfur region. The estimates of child mortality are described based on the age at which a child is exposed to death. Statistical tables showing total births, children surviving and children dead between exact ages (x, x + n) are presented in the tables of analysis. Note that the regional comparisons are made using child mortality estimates from different time points—2004, 2006, and 2007. This does not affect the comparisons since the aim of this research is to understand the influence of conflict on childhood mortality across two different populations. Therefore, childhood mortality comparisons between Southern Sudan and Darfur depend on the experience of each population with respect to conflict, not periods. Only within Southern Sudan do I explore childhood mortality variations with respect to periods. The levels of childhood mortality furnished in this study were obtained using the Brass et al. (1968) method of indirect estimation of child mortality. A chief assumption of this method is that a child’s risk of dying is only a function of the age of that child, and not of any other confounders, such as mother’s age or socio-demographic correlates.
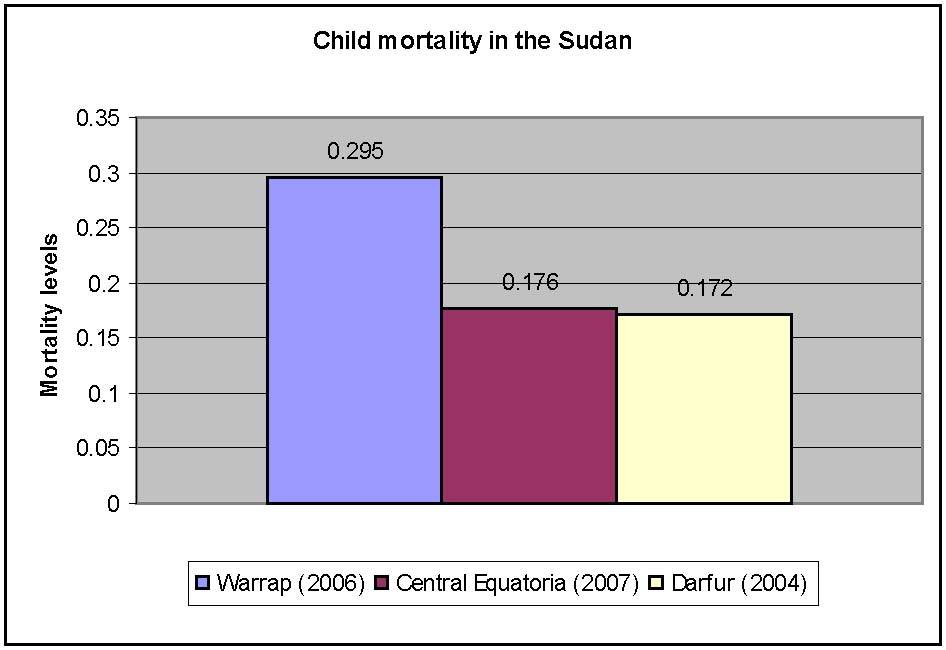
The conflict in Darfur has been characterized as the worst humanitarian crisis of the 21st century. Yet the cross-sectional data indicate higher estimates of childhood mortality in peacetime Thus, my analysis shows that the under-five mortality in Darfur (5q0 = 0.172) is lower than in Warrap state (5q0 = 0.295) and in Central Equatoria state (5q0 = 0.176), both of which are southern states. Figure 1 shows the under-five mortality differentials. Figure 1. Under-five mortality differentials in the Sudan
Numerous justifications are ascertained with respect to the differences my analysis presents. First, child mortality estimates in the Sudan are likely to be influenced by the period of conflict each population experienced. Longer periods of violent conflict imply cumulatively increasing risk of deaths due to direct and indirect causes of violence. This makes much sense in light of the fact that Southern Sudan had experienced over twenty years of violence relative to less than ten years in the state of Darfur. Second, I speculate on the impact of humanitarian effort on survival outcomes in Darfur. Due to a tremendous international outcry with respect to the alleged war crimes in Darfur, many humanitarian services have been directed toward the region. An increase in humanitarian protection programs in Darfur might have led to more human services or resources made available in support of the vulnerable populations. The humanitarian intervention initiatives help provide nutrition and health services, mostly to women and children living in refuge. Finally, variation in the mortality estimates between Southern Sudan and Darfur could likely arise from data uncertainties, though other evidence from the 2006 Household data supports the existence of such differences. Data, specifically from Darfur, are likely to be generated through extrapolation techniques, raising a valid concern of realistic representation. WHO conducted surveys, serving as the principal source of Darfur data, face notable challenges. Palloni and Parker (2006) and Hagan and Rymond-Richmond (2009) noted that health statistics do not incorporate the pre-camp deaths but rather concentrate primarily on disease and nutritional challenges affecting refugees within the settlements. To illustrate the differences, I report the under-five mortality between South Sudan and Darfur as shown in figure 1 above. Mortality due to all causes based on cross-sectional and retrospective data is higher among children in Southern Sudan than in Darfur, other studies show. One year into the most recent violence, Darfur under-five mortality in 2004 was about 2 per 10,000 per day (Grandesso et al., 2004) compared with an extremely high under-five rate of 25 per 10,000 per day in the southern state of Upper Nile in 2002 (Guha-Sapir et al. 2005). While rates of childhood mortality in Darfur seem lower following a year of violence in the region, this difference may be attributed to the level of atrocities experienced during that particular time period. Subsequent studies have shown increased hostilities in the region–an indication of a possible increase in childhood mortality following the referenced year. But evidence shows that the child mortality rate in Darfur remains in its lower trajectory, specifically as it compares to that in southern states. In 2002, for example, child mortality in southern states was high because of epidemics of bloody diarrhea and malnutrition, peaking at about 16 per 10,000 per day in June (Guha-Sapir et al 2005). Along similar lines, UNICEF reported in 2004 that 57 percent of all deaths in Southern Sudan were persons under the age of five. These death estimates illustrate the background for the fact that one out of four newborns in Southern Sudan is likely to die before reaching the age of five. In short, levels of childhood mortality in the south vary substantially by individual state and period, but remain higher than for the rest of the Sudan, particularly Darfur. Variation in childhood mortality in the Sudan is associated with levels of urbanization and development as discussed above. These differences appear even more striking in an Eastern African regional context.
Table 11 shows childhood mortality patterns in Southern Sudan. Results suggest that the probability of dying, q(x), for children of Southern Sudan has recently decreased. Roth and Kurup (1990), using a 1985 sample survey data from Wau and Juba towns, found lower child mortality estimates compared to those reported subsequently by the UN in 2004, though their estimates were relatively higher compared to those reported in 1982 by Preston and Farah. The present study, however, shows that childhood survival in Southern Sudan has improved following the year 2004. This improvement in childhood survival in Southern Sudan is probably due to the 2005 CPA mentioned elsewhere in this paper. The most recent survey conducted in the state of Central Equatoria shows low levels of childhood mortality (see table of results below).
Lower levels of child mortality within these two separate populations vary between 4 percent in Warrap and zero percent in Central Equatoria, respectively. Mortality estimates for children between the ages of zero and one likely stayed lower because women who are newly entering their first marital unions are subjected to sampling data before giving birth to a child, which can influence both the average number of births and proportion of children dead per mother in a specific age category. For persons above the age of one, the levels of mortality increase sharply in both states, supporting the prior argument that the probability of dying for an individual in a population increases with age. This sample property tends to hold for almost all populations analyzed in this fashion. Mortality estimates for people under the age of five hit 29.5 percent in Warrap (2006) and 17.6 percent in Central Equatoria (2007), indicating a greater severity of child mortality in the former than in the latter among those specific ages.
Dramatic reductions are seen in childhood mortality in Southern Sudan. This study shows a significant reduction in childhood mortality from about 56 percent in 2004 according to the UNICEF estimate to 23 percent in the 2007 survey—nearly a 60 percent reduction in mortality rate. I speculate that this changing pattern of child survival is due to the Comprehensive Peace Agreement (CPA), inked in 2005, which ended a twenty-two-year old civil war between southern rebels and the northern regime. The peace agreement might have led to a significant reduction in overall deaths as well as to improved human services in the region, which consequently lessened the degree of childhood mortality associated with malnutrition, infectious diseases, and of course, violence. This short period of relative peace might have created other incentives for a majority of the southern population who live in major towns. After the signing of the peace agreement, increased proportions of regional reconstruction funds and related aid from donor communities have been specifically channeled to major towns in Southern Sudan. In addition, the autonomous government of Southern Sudan (GoSS) gained full participation in the central government, and an annual financial share of one billion dollars for the southern region. This increase in revenues in the region may have consequently contributed to rejuvenation of the major regional social systems through, among others, reconstruction of inter-nation roads, rebuilding of agricultural sectors, and reconstruction of health and business industries. The peaceful period enabled by the agreement has also attracted international businesses to the region, making transfers of business supplies and services from neighboring countries to the region more feasible than during the war. These business relations between Southern Sudan and other nations have boosted regional economic growth, as well as enabling public accessibility to basic human services. Another byproduct of peace which boosts survival improvements in Southern Sudan is an enabled submission of remittances through international banking systems by south Sudanese who live in the Diaspora. After the CPA, thousands of Southern Sudanese who found refuge in industrialized societies during the period of conflict started, in support of their families, to send millions of dollars to Southern Sudan each year. These funds increase the spending power of individual families thereby contributing to regional economic growth, as well as improving their living conditions at large. UN services in conflict confronted populations are conditional on the complex security situations those populations experience. Generally, the United Nations plays a tremendous role in reducing or preventing deaths linked to disease and malnutrition among persons stranded in refugee or displacement settlements, but based mostly on the security atmosphere of conflict areas in which those services are sorely needed. The United Nations has been involved in Sudan since the 1980s, providing humanitarian aid to those affected by wars in all accessible corners of the Sudan. I speculate that UN services were not as effective in Southern Sudan and elsewhere in the country during the conflict due to complex conditions of war, among others. Rather, humanitarian services to war victims in the Sudan seem to have been largely confined to populations residing in minimally secure locations, such as displacement camps or settlements, especially in neighboring nations. This concentration of UN services in specific areas, as a function of security measures, may have made it difficult for Sudanese who were stranded in worst security zones to receive needed aid from the UN and from related humanitarian agencies. Thus, the improving security situation owing to the peace agreement in the region might have boosted UN efforts to ensure effective delivery of human services to the needy, the majority of them children. Perhaps services—including child immunizations, feeding programs for malnourished children, and provision of clean water—were more effectively distributed following the peace agreement. In short, improved political and security situations in Southern Sudan, seem to have accounted for improvements in regional economic and health conditions, possibly allowing for effective provision of human services in the region. In particular, these changes may account for improved standards of living through reduced health disparities, mostly for women and children under the age of five whose population represents a large proportion of vulnerable persons.
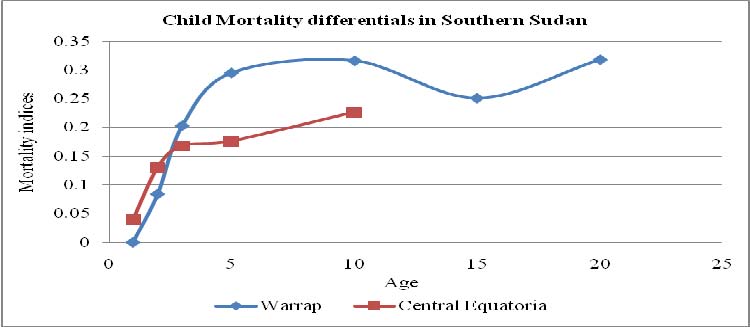
Estimates of childhood mortality in Southern Sudan vary markedly across states. As shown in Figure 1, child mortality estimates are higher for the state of Warrap and lower for the state of Central Equatoria as illustrated elsewhere in this study. Major factors influencing this variation in childhood mortality include the state’s level of urbanization, access to commercial resources, and maternal education levels. Figure 2. Childhood Mortality Differentials in Southern (2006 and 2007)
Although Southern Sudan as a whole is widely known for its highly disabled infrastructure due to war, the worst scenarios of this kind seem to be concentrated in particular states. Research suggests that, compared to Central Equatoria, Warrap state exhibits the poorest infrastructure and very frail social and economic development. These factors are coupled with successive civil wars and historical under-development, frustrating human progress in Southern Sudan. The state of Warrap, however, has never experienced development, even prior to the civil wars. Three years into the peace agreement, Warrap state’s system remained under-developed, which perpetuates insecurity in the state’s economic, social, and political life. Central Equatoria, by contrast, is far better off than most other southern states in nearly all aspects of social development and infrastructure. Before the recent civil war, trajectories of slow, but progressive development in Central Equatoria state were planted as far back as colonial times, especially at times during which it was made a center of colonial government for the southern portion of the country. Changing economic, health, and educational systems in Central Equatoria appeared as far back as the late 1970s and the early 1980s when the Sudanese central government started to build various institutions in the region as a result of the 1972 peace agreement. For instance, Juba, the state capital of both Southern Sudan and Central Equatoria, became a site of South Sudan’s first national university in 1977. Improved commercialization in Central Equatoria is also owed to the presence of market amenities in the town of Juba. Coupled with existing political relations between East African countries and Southern Sudan as a whole is regional trade. Central Equatoria’s proximity to neighboring Kenya and Uganda enables commercial interactions among the populations. These business relations, in turn, create accessibility to food and medical imports for persons living in Central Equatoria. Further, using the data that I collected in 2006 and 2007, I also compared Warrap State and Central Equatoria within the Southern Sudan, evaluating that the differences in childhood mortality across these southern states are not due to chance. At a 90 percent confidence level with 1 df, I obtained a chi-square value of approximately 0.038 (p = .10, N = 1,490). I conclude that a chi-square of approximately 0.038—which is significant at the 0.05 level—is too large to have arisen by chance, and is likely to reflect real differences between the two southern populations. The coefficient of variation calculated as the ratio of standard deviation to the average number of dead children in each setting revealed a consistent story. These measures are in form of natural log and include 65 percent in Central Equatoria and 81 percent in Warrap, signifying a greater relative variability in the latter than in the former. In other words, the mortality rate was 21 percent in Warrap State and 17 percent in Central Equatoria.
In this paper, I used 2006 Sudanese household sample and 2006 and 2007 sample data from Warrap and Central Eqautoria to study child mortality differentials across Sudanese states. This paper has specifically mapped out how the patterns of childhood mortality and development and mortality indicators differ across Sudanese regions. Findings are remarkable and in direction of the initial expectations. Results show that of the studied Sudanese states, South Sudan has the highest mortality levels. Child mortality patterns in the Sudan are generally influenced by numerous development indicators/disequilibrium in resource distribution, protracted periods of conflict, instability, and maternal years of schooling. A significant association between child mortality regime and conflicts is evident. For example, the child mortality rate in Southern Sudan was relatively lower in 1982, higher in the 1990s through 2004, and lower again in 2005 to present. Proliferated child mortality levels in Southern Sudan in the 1990s indicate the effects of civil conflict which started in 1983 and ended in 2005. The results of the 2006 and 2007 sample surveys indicate that childhood mortality in Southern Sudan has recently declined–showing a significant drop from the UN reported 56 percent in 2004 to approximately 23 percent in 2007. These dramatic reductions have a probable association with the Sudanese Comprehensive Peace Agreement signed in 2005. The peace agreement virtually ended the protracted violence, consequently curtailing the excess mortality linked to violent deaths, while allowing for effective delivery of needed health and nutritional services to children in Southern Sudan. Child mortality levels vary markedly across southern states, with a relatively higher pattern in Warrap State than in Central Equatoria State. Everything else being equal, child mortality conditions across Southern Sudan states are also associated with the levels of urbanization, access to commercial resources, instability, and historical development. For instance, low rates of childhood mortality in Central Equatoria could be related to its relatively developed social and economic infrastructures, which support both local and international economies. Notwithstanding the detrimental effects the current political crisis might have had on Darfur, evidence suggests that Southern Sudan continues to experience a comparatively higher rate of childhood mortality. But the absence of complete child mortality data for Darfur prevents a thorough comparison of child mortality patterns among all ages across the states. Thus, in this paper, child mortality rates for the two regions were compared only for persons under the age of five, based on the available data during different time points. And according to the estimates, under-five mortality is comparatively lower in Darfur than in Southern Sudan. Evidence from 2006 household data paints a more complete picture regarding these childhood mortality differences: Southern Sudan continues to trail nearly all states of the Sudan with respect to development and availability of human services which are used as proxies of general population health. In addition, substantial differences in the experience of human populations in the Sudan may also be understood through an evaluation of expectation of life at birth of an overall population. For instance, in the period 1955-1973, life expectancy at birth was quite lower in the south relative to other regions or states of the Sudan. In particular, expectation of life at birth was 36 years in the south vis-à-vis 48 years in Darfur and 52 years in the northern state of Khartoum in 1973 (Preston and Farah 1982). The social and political conditions, which explain the actuarial state of the Sudanese populations, have not yet witnessed major transformations, not even in recent years, especially in Southern Sudan. Estimates of childhood mortality in a region that continues to face turmoil are largely constrained by the complex conditions of war, which adversely affect reliable methods of exploration. This is particularly the issue in Darfur, where most death estimates come from conjectural paradigms. There is also good reason to believe that the child mortality estimate in 2004 in the state of Darfur possibly down-biases the overall child mortality experience of the region. The estimator represents the earliest rather than the latest conditions of conflict and child mortality in the region. Similarly, rates of childhood mortality in Darfur may be subject to various sampling and reporting errors, problems that are apparent across various studies concerning death counts in the region. Estimating mortality in war zones generally poses an enormous challenge, as the complex conditions of war tend to inherently weaken the methodological rigor underlying the study. The data used here are not without vices. Sample selection—specifically in the case of Warrap and Central Equatoria data gathering—was problematic. Conveniently accessible subjects—rather than randomly selected subjects—were recruited for this study. This constrained diversity in the outcomes, resulting in somewhat homogeneous sample points. Other restrictions pertaining to how the data were obtained are analytically problematic. These restrictions also lead to selection biases, which have no current solutions in nations with extremely poor record keeping conditions. First, the indirect estimation techniques restrict sampling to married women aged 15 to 49. This creates bias because children of unmarried, younger, or older mothers are excluded. The second restriction is that only surviving, married women were allowed to take part in the study. Although this is done to explicitly avoid sampling errors resulting from misreporting of historical births to deceased mothers, the demerit of the procedure is that it creates downward bias of children’s death estimates. Age of mothers at the time of survey presents an additional challenge for this study. Many women born in rural areas of Southern Sudan have no birth records and are usually unable to accurately track their exact dates of birth. Though I framed some baseline standards for inferring their exact ages, still some uncertainties are likely to arise in the reporting. For women who have no birth records, I adopted two standards: I estimated the average age of each mother based on the standard average age at first marriage and the reported length of time in years each woman has spent in marriage, which was known to majority of women. In Sudanese society, most women enter their first marriage around the age of 15 years old, with probably a modest variation between urban and rural populations. Although rural-born Sudanese women tend to be quite uncertain in reporting their exact ages at birth, the majority tend to remember the length of time they have spent in marriage. As proxies for estimating women exact ages during the period of sampling, a woman who reported having been in a marriage for an x number of years received (15 + x) as their final estimated age at the time of survey. The strategy is the best possible there is to this problem, though no one could optimistically and realistically assure full accuracy of the information collected in relation to participants’ exact ages. This study is significant both from policy and from future academic research standpoints. The research is useful with respect to Sudanese policy developments in public health, infrastructure, security, and political economy. These factors account for majority of the social and health consequences, as well as the life outcomes the country experiences. These forces require improvements in order to reverse the living conditions of the citizens, particularly the Southerners and Darfuris. The research also serves as a blueprint or point of departure for future demographic studies in the Sudan, particularly in Southern Sudan.
**The analysis evaluates these indicators on a mixed basis of both geographic and geopolitical categorization of the regions, particularly the North, East, and Eastern states. Geopolitically, East Sudan is made up of four states, including Gezira, Sennar, Blue Nile Central, and White Nile. Geographically, a combination of eastern and northeastern states—such as Kassala, Al Qadarif, and Red Sea—forms the Eastern region. Geographically, the Northern region consists of Khartoum, North, and River Nile states; geopolitically, this extends further to the Northeast and Eastoern regions.
Brass, W., et al., The Demography of Tropical Africa. 1968: Princeton University Press. Farah, A.-A. and S.H. Preston, Child Mortality Differentials in Sudan. Population and Grandesso, F., et al., Mortality and Malnutrition Among Populations Living in South Darfur, Guha-Sapir, D. and O. Degomme, Darfur: Counting the Deaths. 2005. Guha-Sapir, D., O. Degomme, and V. Teran, Civil Conflicts in Four African Countries: A Five- Hagan and Rymond-Richmond (2008). The Collective Dynamics of Racial Dehumanization and Genocidal Victimization in Darfur. ASR, 2008. 73(6): p. 875-902. Hagan and Rymond-Richmond (2009). Darfur and the Crime of Genocide. Cambridge University Press. Hill, K. and A. Pebley, Child Mortality in the Developing World. Population and Development Lorimer, F., Demographic Information on Tropical Africa. 1961: Boston University Press. 7-9. Maglad, N., Fertility in rural Sudan: The Effect of Landholding and Child Mortality. Economic Palmer, C., L. Lush, and A.B. Zwi, The emerging international policy agenda for reproductive Rice, A., et al., Malnutrition as an underlying cause of childhood deaths associated with Roth, E. and K.B. Kurup, Child Mortality Levels and Survival Patterns from Southern Sudan. Singh, K., et al., Forced Migration and Under-five Mortality: A Comparison of Refugees and Tarver, J.D., The Demography of Africa. 1996: Praeger Publishers. 49-51, 60-62. WHO and UNICEF (2007). Levels and Trends of Child Mortality in 2006. A Working Paper. UNICEF (2007). The State of the World’s Children: Child Survival. An Annual Report. United Nations, Indirect Techniques of Demographic Estimation. 1983: United Nations. 73-81. Zachariah, K.C. and S.H. Soliman, Use of Population and Housing Survey Data of the Sudan for
|







Makol Ariik Development Foundation © 2007 | Privacy Policy
Website by Leah Martin